
Back in the 1990s, the state was facing a Medicaid problem similar in size and scope to the one Pat Quinn addressed in his budget speech this week. The problem, and one of the proposed solutions, should sound familiar:
[Then-Secretary of State George] Ryan's plan, for which he acknowledged no bill has been drafted and no sponsor found, calls for putting five floating casinos in Chicago, three in suburban Cook County and two in Lake County. A similar plan to double the number of casinos plying Illinois waters has been floating around the Capitol since last year.
In addition, he proposed raising the state tax on the adjusted gross receipts of riverboat casinos to 25 percent from 20 percent, and he called for a 5 percent tax on any boat's adjusted gross income above $100 million annually.
Ryan said the extra $1.5 billion that the tax would generate over four years should be earmarked to erase a Medicaid debt of $1.4 billion.
Five floating casinos in Chicago. Needless to say, this didn't happen.
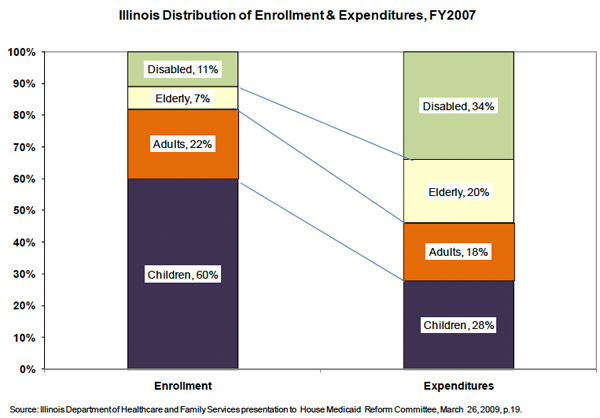
One of the issues with the state's Medicaid spending that experts have addressed is the amount spent on the elderly and disabled. More than half the state's Medicaid spending goes to those groups, even though they make up less than a fifth of recipients.
To control or cut Illinois' Medicaid costs, the state must focus on disabled and elderly patients instead of welfare families, a group of health researchers said Wednesday.
Medicaid expenses for disabled and elderly patients hit nearly $3.2 billion, representing about 66 percent of Illinois' $4.7 billion Medicaid cost, in the state's last budget year.
Yet the state has not devised a strategy for controlling those costs, according to the study, released by the University of Chicago's Center for Urban Research and Policy Studies.
Instead, the researchers noted, Gov. Jim Edgar's proposed managed-care plan for Medicaid, currently awaiting federal approval, is targeted primarily at welfare patients whose medical expenses represent less than one-third of the overall Medicaid costs.
So what happened to the crisis? Unpopular reimbursement cuts reduced expenses, and an improving economy backed Illinois off the ledge. Jim Edgar's MediPlan Plus push towards managed care—estimated by U. of C. critic Henry Webber to save no more than a range of five to 15 percent of costs—faded away. But the structural problems remained, and in a down economy, they're impacting the budget in a big way. Over at Capitol Fax, Rich Miller has a good roundup of stories that's well worth your time. In particular, Carla Johnson's piece, which includes comments from Quinn senior medical adviser Michael Gelder is excellent, and covers some of the emerging details on the menu:
The list also include more drastic cuts, such as changing eligibility rules for nursing homes and at-home help so that some incontinent elderly people who can't prepare their own meals would be denied state-financed care.
[snip]
Increasing the cutoff score, as proposed, would mean people such as a 65-year-old incontinent woman with cataracts and arthritis who needs help with cooking and taking medications would no longer qualify for Medicaid help at home, said Carol Aronson of Shawnee Alliance in Carterville, which does such evaluations for the state.
Related: Another angle to the elderly-care issue in Illinois was addressed back in 1988, as these problems were starting to build. In the Journal of Applied Gerontology, researchers from the University of Michigan, the Gerontological Society of America, and the University of Illinois at Chicago compared Michigan's approach (focused on paid but informal caregivers) with Illinois's (agency focused). While I haven't had time to consider it fully, it's an interesting read:
A 1985 evaluation of the Michigan program provides evidence that informal caregivers provide clients more regular, consistent, and reliable care (Michigan Department of Social Services, 1985; Nye, 1985). In initiating competitive bidding among contractors, Illinois stimulated a significant turnover in agency contracts in fiscal years 1984 and 1985, affecting a substantial proportion of the program’s clients. Stabiliy of the caregiving relation was more assured by the Michigan program’s contracting with informal caregivers.
Photograph: erix! (CC by 2.0)